Health education & navigation only. CareBridge is NOT a medical practice. The Health Navigator is not registered with AHPRA or the Medical Board of Australia. Nothing on this page or provided by CareBridge constitutes medical advice, diagnosis, or treatment recommendation. All clinical decisions remain with your treating registered health practitioner. Medical emergency: call 000.
What is POTS & Dysautonomia?
Postural Orthostatic Tachycardia Syndrome (POTS) is a form of dysautonomia — a disorder of the autonomic nervous system — characterised by an abnormal increase in heart rate of 30 beats per minute or more (40+ bpm in adolescents) within 10 minutes of standing, in the absence of orthostatic hypotension. It affects an estimated 1–3 million people in the United States alone and is increasingly recognised in Australia.
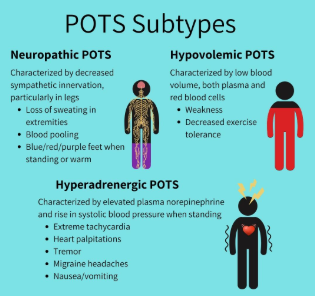
POTS is not a single disease but a syndrome with multiple subtypes including hypovolemic POTS, hyperadrenergic POTS, and neuropathic POTS. It frequently co-occurs with other connective tissue and autoimmune conditions, particularly Hypermobile Ehlers-Danlos Syndrome (hEDS) and Mast Cell Activation Syndrome (MCAS).
POTS became more widely recognised following the COVID-19 pandemic, as a significant subset of post-COVID (long COVID) patients present with new-onset POTS or dysautonomia symptoms.
How does it get recognised?
POTS is diagnosed based on a documented heart rate increase meeting published criteria upon standing, combined with typical symptoms. Many patients are told their symptoms are anxiety or deconditioning before a POTS diagnosis is considered.
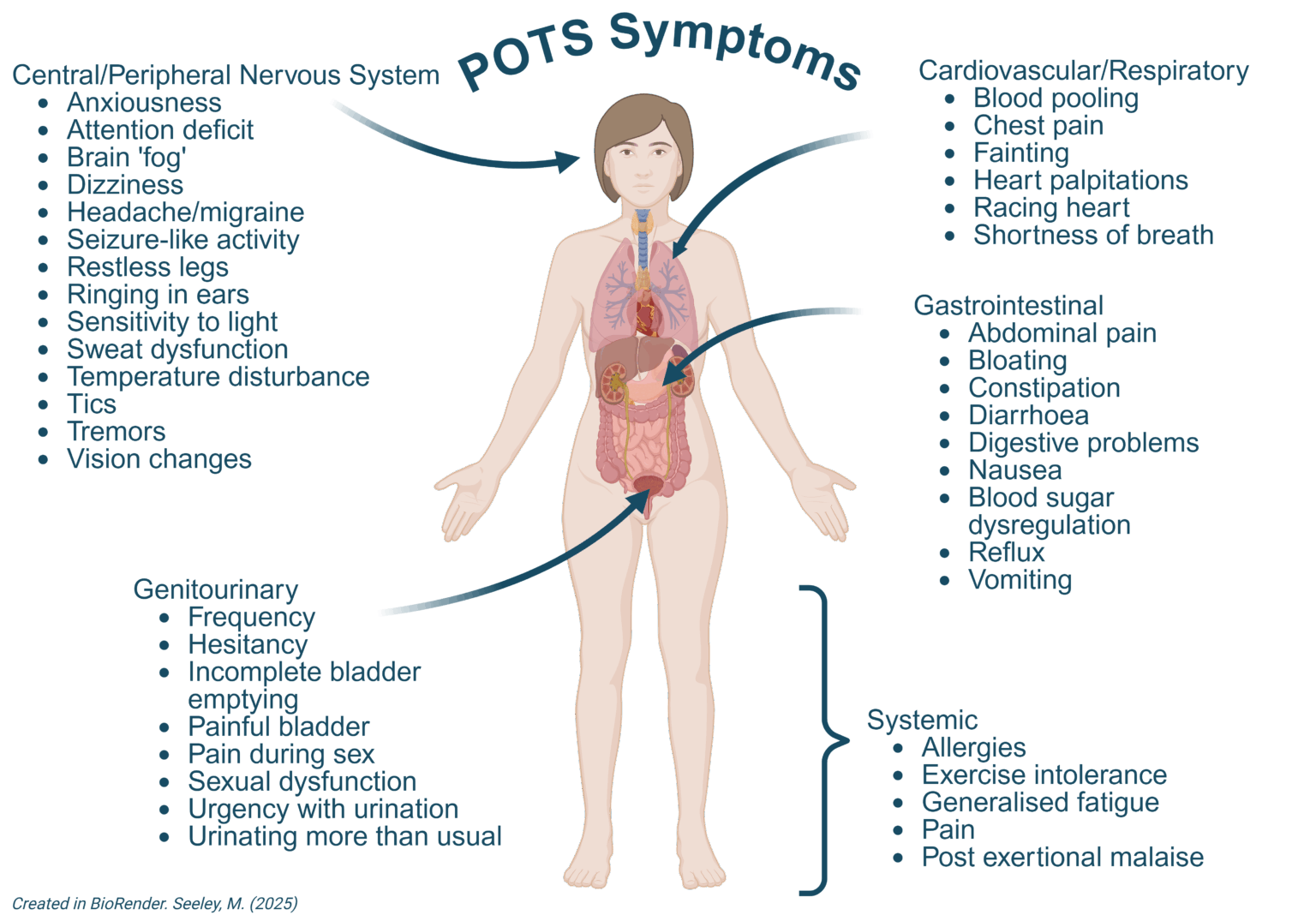
Common reported symptoms:
- Rapid heart rate (palpitations) when standing
- Dizziness, lightheadedness, or pre-syncope on standing
- Extreme fatigue — worsened by upright posture
- Brain fog and cognitive difficulties
- Headaches, especially positional
- Shortness of breath on minimal exertion
- Nausea and GI symptoms
- Temperature dysregulation and sweating abnormalities
- Exercise intolerance
- Near-fainting or fainting episodes
- Visual disturbances when standing
- Chronic pain
Why does it take so long to get answers?
POTS is under-diagnosed in Australia for several reasons. Its symptoms — dizziness, fatigue, brain fog, palpitations — are non-specific and overlap with anxiety, deconditioning, and chronic fatigue. Many GPs are not familiar with the NASA Lean Test (active stand test), which can be performed in-office and is the first step in POTS evaluation.
The diagnostic pathway typically requires a GP referral to cardiology for tilt table testing, and cardiologists often do not see POTS as a primary concern. The result is that many patients spend years being told their symptoms are psychosomatic before receiving a correct evaluation.
How is it currently diagnosed in Australia?
In Australia, POTS is most commonly evaluated via the active stand test (NASA Lean Test) at the GP level — checking heart rate in the lying and standing position at intervals over 10 minutes. This requires no specialist equipment and can be requested at a routine GP visit.
Formal diagnosis is typically confirmed by a cardiologist via tilt table testing, in which the patient is tilted from lying to standing on a motorised table while heart rate and blood pressure are continuously monitored. Cardiology referral from a GP is required and is Medicare-rebatable.
Additional investigations may include 24-hour Holter monitoring, blood volume studies, and blood tests to rule out other causes of tachycardia.
How CareBridge helps
CareBridge prepares a structured document for your GP that presents your reported symptoms mapped to the published POTS diagnostic criteria from the Heart Rhythm Society (2015) and the American Autonomic Society. The document includes a suggested investigations table (active stand test, 24-hour Holter, relevant blood tests) and a request for cardiology referral — framed in clinical language that reduces the risk of dismissal.
For patients who have already been told their symptoms are anxiety or deconditioning, a Tier 2 or Tier 3 report includes a dedicated section on the published literature distinguishing POTS from anxiety, including studies on post-viral POTS onset where relevant.
View report tiers and pricing →