Health education & navigation only. CareBridge is NOT a medical practice. The Health Navigator is not registered with AHPRA. Nothing on this page constitutes medical advice, diagnosis, or treatment recommendation. All clinical decisions remain with your treating registered health practitioner. Medical emergency: call 000.
What is Ehlers-Danlos Syndromes?
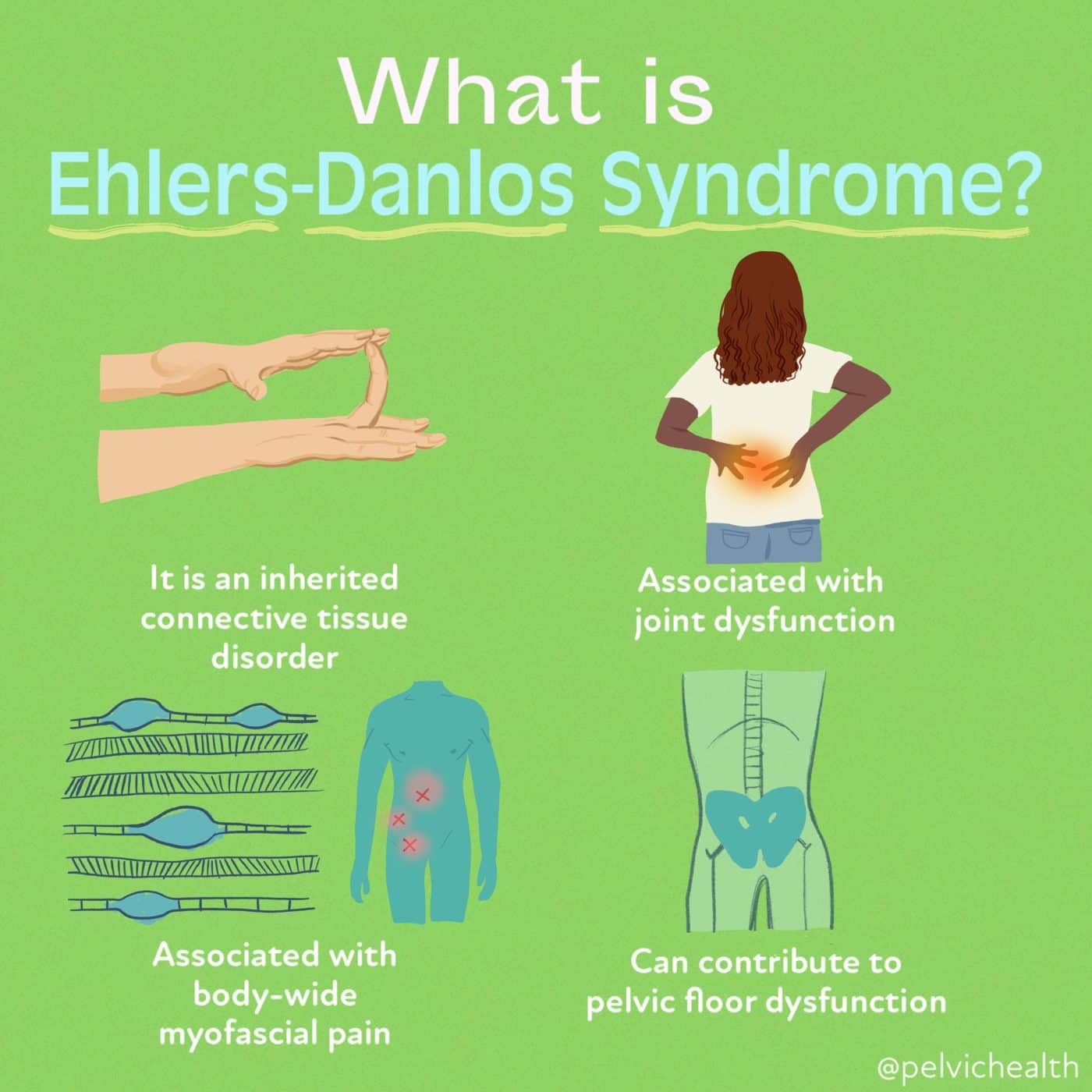
Ehlers-Danlos Syndromes (EDS) are a group of hereditary connective tissue disorders characterised by joint hypermobility, skin hyperextensibility, and tissue fragility. There are 13 recognised subtypes with distinct genetic causes. Hypermobile EDS (hEDS) is the most common and is the only subtype without a confirmed genetic marker, making clinical diagnosis essential.
EDS affects connective tissue throughout the body — tendons, ligaments, skin, blood vessels, and internal organs. As a result, it is a multi-system condition that can affect joints (dislocations, subluxations), skin (easy bruising, delayed healing), the cardiovascular system (through POTS), the digestive system, and the immune system (through MCAS).
EDS frequently co-occurs with POTS and Mast Cell Activation Syndrome (MCAS), a triad known informally as the "POTS-hEDS-MCAS trifecta." Recognition of this overlap is important for comprehensive evaluation.
How does it get recognised?
EDS is diagnosed clinically, as most subtypes have now been confirmed with genetic testing — with the critical exception of hEDS, which is diagnosed based on the 2017 International Classification criteria. This requires a physical examination by a knowledgeable clinician and a thorough history.
Common reported symptoms:
- Joint hypermobility (Beighton score ≥ 5/9)
- Recurrent joint dislocations or subluxations
- Chronic widespread joint and muscle pain
- Soft, velvet-like or hyperextensible skin
- Easy bruising without injury
- Delayed wound healing or abnormal scarring
- Chronic fatigue
- POTS-type symptoms (dizziness on standing)
- Gastrointestinal dysmotility — nausea, bloating
- Pelvic floor dysfunction
- Anxiety and autonomic symptoms
- Proprioceptive difficulties — clumsiness or poor balance
Why does it take so long to get answers?
EDS is under-diagnosed for multiple reasons. Most GPs are not trained to perform or interpret the Beighton score, and widespread hypermobility is often dismissed as "just being flexible." The multi-system nature of EDS means patients present to different specialists for different symptoms without anyone connecting the dots.
In Perth, rheumatology has the longest wait times of any specialty — often 12–18 months for a new patient appointment. Without a strong referral letter presenting the case clearly, many patients are not prioritised or are discharged without evaluation for EDS specifically.
How is it currently diagnosed in Australia?
hEDS is diagnosed using the 2017 International Classification criteria, which require assessment across three categories: generalised joint hypermobility (Beighton score), systemic manifestations of connective tissue disorder, and exclusion of other heritable connective tissue disorders. A GP can initiate the Beighton score assessment.
For other EDS subtypes, genetic testing is available through clinical genetics services in Australia via a GP or specialist referral. The Perth Children's Hospital clinical genetics service and PathWest laboratories both offer relevant testing panels.
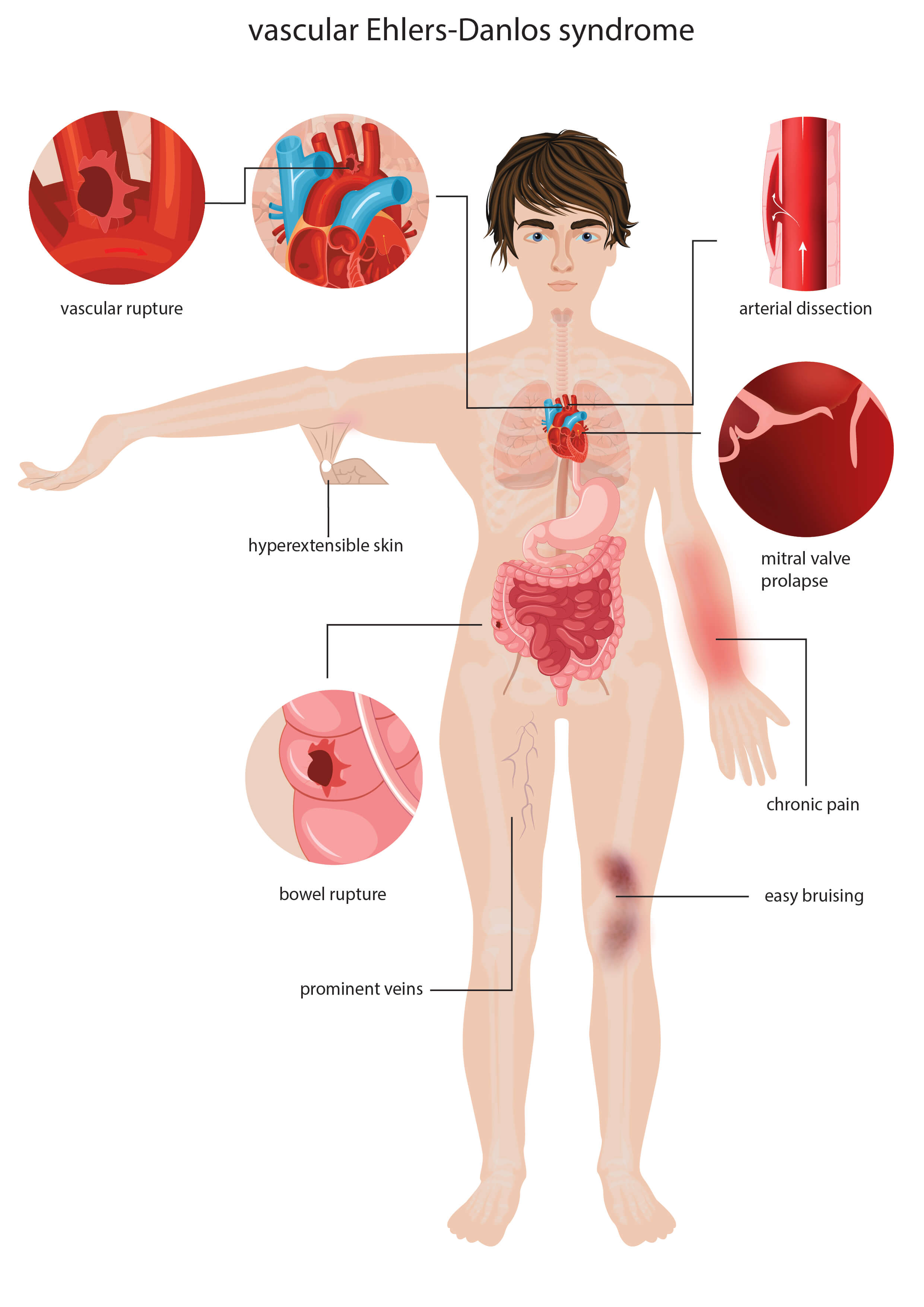
Additional investigations commonly required include echocardiogram (vascular EDS screening), skin biopsy (for classical EDS), and multidisciplinary assessment for pain management and physiotherapy.
How CareBridge helps
CareBridge prepares a structured report mapping your reported symptoms to the 2017 hEDS classification criteria and presenting the published literature on EDS-POTS-MCAS overlap where relevant. The report is designed to support a rheumatology referral — framed around what a Perth rheumatologist needs to see to prioritise the appointment and conduct a targeted evaluation.
For complex cases involving multiple co-occurring conditions, a Tier 3 report covers all relevant conditions with separate evidence sections and a specialist referral pathway for each — reducing the number of separate appointments and documentation patients need to manage independently.
View report tiers and pricing →